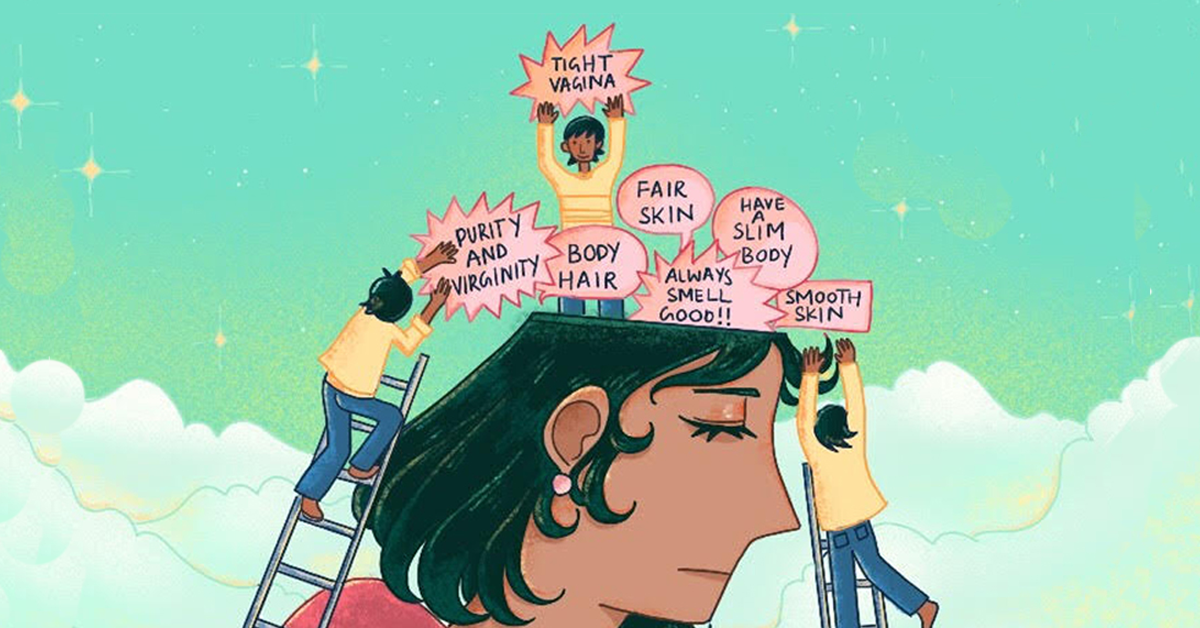
Dr Anamika PradhanIllustrated by Maddox Pazl A doctor asks: can we please have conversations around (hetero)sexual pleasure that don’t focus on ‘editing’ women’s bodies for men’s sake?The other day, I got a text message from a friend that really made me sit up!It was a link to an ad by a doctor who was openly advertising some incredible ‘services’. “Complete re-virgination akin to 16 year old girl” (Rs 65,000), “Hoodectomy for more sexual pleasure” (Rs 20,000), and “Superfemale with superhymenoplasty” (Rs 1,15,000) were just some of the items on his list – with prices in rupees and dollars. Out of the kindness of his heart, it appears, he also offers a heavy discount.Ironically, the friend who told me about him is a filmmaker who has been working on mobilising women to speak out against khatna, the female genital mutilation (FGM) which is being practised in India for religious and cultural reasons, and which aims to control female sexuality. And here was a member of the medical profession advertising for more unnecessary procedures involving women’s genitals, claiming it would lead to pleasure – but for whom? There is a clue here: the doctor in question also offers a training programme and has published an article in a journal which starts like this: “Hymenoplasty is required to restore the hymen if torn before marriage. Nowadays hymenoplasty is also requested by some females at their 25th anniversary to be enjoyed as re-virgin.” While one may be inclined to dismiss this as an individual case, the shocking reality is that this doctor isn’t the only one of his kind. There’s a growing medical-corporate-pharma complex that feeds into people’s insecurities and upholds patriarchal ideas of what is appropriate for women’s bodies. It starts off with the insidious and all-pervasive suggestion to be ‘fair and lovely’ and then moves on to the need to have flawless skin, no body hair but luxurious hair on your head, smell like a flower, be slim and always be attractive to men. But it doesn’t end with just a focus on external appearance.There is a vaginal ‘tightening’ product called 18 Again that was advertised for a brief while and still continues to be sold. It talks about how it makes the sex feel like the “first time every time”. It also claims to include gold among its ingredients, as well as Punica Granatum, about which it says on its website: “According to a legend, Punica Granatum grew in the Garden of Eden and the fruit has been used as a folk medicine for thousands of years.” Of course there are plenty such ‘snake oil’ variations being sold to gullible people, but this one actually has gynaecologists endorsing it on their website.Setting aside the tall claims of such products, what is so exciting about a woman’s ‘first time’ that one can market that as something worthwhile? Who is a ‘tight’ vagina meant to be pleasurable for? Clearly, for her male partner. How can we have a conversation about women’s sexual pleasure without talking about a range of topics such as foreplay, relationships issues, male erectile dysfunction? Even the medication for male erectile dysfunction gets marketed as something that will help men regain sexual pleasure, not for women whose partners are unable to get it up!If society, with the premium it places on “purity” and virginity, sees women’s sexuality through the lens of male pleasure and is okay with asking women to do unreasonable things to their bodies, doctors are caught in this cultural web too. The reality is that in 5 years of MBBS and 3 years of post-graduate training (whether in ObGyn or any other field), there is no formal training on issues of sexual health. When it comes to women, the entire focus is on reproduction and in managing pathologies like menstrual disorders and other conditions. The biology of pleasure does not figure in understanding women’s bodies, and this is a cultural bias that shapes the medical field.Has anyone looked at the textbooks we learn from? One of the forensic medicine textbooks defines a virgin as “a female upon whose body the sex act has not been performed” – so only women are virgins, and their role in sex is seen as a passive one, of receivers, not participants. Forensic medicine deals with medico-legal cases (such as rape), and thus this kind of mindset is disturbing.
While one may be inclined to dismiss this as an individual case, the shocking reality is that this doctor isn’t the only one of his kind. There’s a growing medical-corporate-pharma complex that feeds into people’s insecurities and upholds patriarchal ideas of what is appropriate for women’s bodies. It starts off with the insidious and all-pervasive suggestion to be ‘fair and lovely’ and then moves on to the need to have flawless skin, no body hair but luxurious hair on your head, smell like a flower, be slim and always be attractive to men. But it doesn’t end with just a focus on external appearance.There is a vaginal ‘tightening’ product called 18 Again that was advertised for a brief while and still continues to be sold. It talks about how it makes the sex feel like the “first time every time”. It also claims to include gold among its ingredients, as well as Punica Granatum, about which it says on its website: “According to a legend, Punica Granatum grew in the Garden of Eden and the fruit has been used as a folk medicine for thousands of years.” Of course there are plenty such ‘snake oil’ variations being sold to gullible people, but this one actually has gynaecologists endorsing it on their website.Setting aside the tall claims of such products, what is so exciting about a woman’s ‘first time’ that one can market that as something worthwhile? Who is a ‘tight’ vagina meant to be pleasurable for? Clearly, for her male partner. How can we have a conversation about women’s sexual pleasure without talking about a range of topics such as foreplay, relationships issues, male erectile dysfunction? Even the medication for male erectile dysfunction gets marketed as something that will help men regain sexual pleasure, not for women whose partners are unable to get it up!If society, with the premium it places on “purity” and virginity, sees women’s sexuality through the lens of male pleasure and is okay with asking women to do unreasonable things to their bodies, doctors are caught in this cultural web too. The reality is that in 5 years of MBBS and 3 years of post-graduate training (whether in ObGyn or any other field), there is no formal training on issues of sexual health. When it comes to women, the entire focus is on reproduction and in managing pathologies like menstrual disorders and other conditions. The biology of pleasure does not figure in understanding women’s bodies, and this is a cultural bias that shapes the medical field.Has anyone looked at the textbooks we learn from? One of the forensic medicine textbooks defines a virgin as “a female upon whose body the sex act has not been performed” – so only women are virgins, and their role in sex is seen as a passive one, of receivers, not participants. Forensic medicine deals with medico-legal cases (such as rape), and thus this kind of mindset is disturbing. Doctors are taught to do the ‘two-finger test’ (based on the scientifically incorrect idea that a tight vagina indicates that someone hasn’t had sex before, while a lax one means a woman is ‘habituated to sex’) for ‘proof’ of rape in a victim. The logic is that if you are a woman who is used to having sex, then you probably weren’t actually raped. Despite changes in guidelines for examining victims of sexual assault and a Supreme Court ban on the test in 2013, many doctors still continue to use the ‘two-finger test’. Only in May 2019 did Maharashtra remove it from medical textbooks and it is probably the only state to have done so.How does one make the transition from being a 19-year-old fresh medical student who is being taught this, day in and day out, and is studying this and needing to write this as an answer in an exam, to becoming a 27-year-old practising doctor who will be able to recognise that this is objectification and derogatory and that ‘virgin’ is not even a medical topic but a socio-cultural concept created by patriarchy to control women’s sexuality? That, it really has no place in a medical syllabus or application?It is a tough journey to make and most never even bother to think that deeply beyond the overwhelming amount of bio-medical information they need to learn, in the absence of any social and cultural contexts or gender and rights sensitisation.It is a sign of the changing times that there is currently, quite rightly, much being written about the judgemental attitudes of doctors (especially gynaecologists) towards women and their sexual lives.
Doctors are taught to do the ‘two-finger test’ (based on the scientifically incorrect idea that a tight vagina indicates that someone hasn’t had sex before, while a lax one means a woman is ‘habituated to sex’) for ‘proof’ of rape in a victim. The logic is that if you are a woman who is used to having sex, then you probably weren’t actually raped. Despite changes in guidelines for examining victims of sexual assault and a Supreme Court ban on the test in 2013, many doctors still continue to use the ‘two-finger test’. Only in May 2019 did Maharashtra remove it from medical textbooks and it is probably the only state to have done so.How does one make the transition from being a 19-year-old fresh medical student who is being taught this, day in and day out, and is studying this and needing to write this as an answer in an exam, to becoming a 27-year-old practising doctor who will be able to recognise that this is objectification and derogatory and that ‘virgin’ is not even a medical topic but a socio-cultural concept created by patriarchy to control women’s sexuality? That, it really has no place in a medical syllabus or application?It is a tough journey to make and most never even bother to think that deeply beyond the overwhelming amount of bio-medical information they need to learn, in the absence of any social and cultural contexts or gender and rights sensitisation.It is a sign of the changing times that there is currently, quite rightly, much being written about the judgemental attitudes of doctors (especially gynaecologists) towards women and their sexual lives. The Supreme Court may have declared the right to privacy, but when will the medical profession learn to respect the privacy and the personal spaces and sexual choices of women? When will medical textbooks stop talking of virginity and two-finger tests and include discussion on the social, cultural and religious environment within which health and health seeking is practised?The medical and nursing professions should ideally be at the forefront of enabling such social change, since they bear witness on a daily basis to the violations that women and young girls face as a result of archaic and oppressive gender norms. Medicine could be a discipline which makes us see human beings afresh, and opens up our mind to human life in a more realistic way, helping us be better doctors who help people be healthier in a holistic way.We know that beauty is only skin deep, but the misogyny surrounding it and self-hate it creates can cut us right down to our bones, as do harmful ideas about women’s bodies and women’s sexuality, which deeply impact mental health and in turn the overall health of people. If doctors’ goal is to provide healthcare to women, then it’s time they actually focus on women’s health and women’s rights, not damaging women’s minds and bodies for some misguided cultural ideals. Dr Anamika Pradhan is a practising specialist in Mumbai who has studied at one of the medical colleges in the city and feels strongly about the need to produce more humane and thoughtful doctors who can be agents of change in society.
The Supreme Court may have declared the right to privacy, but when will the medical profession learn to respect the privacy and the personal spaces and sexual choices of women? When will medical textbooks stop talking of virginity and two-finger tests and include discussion on the social, cultural and religious environment within which health and health seeking is practised?The medical and nursing professions should ideally be at the forefront of enabling such social change, since they bear witness on a daily basis to the violations that women and young girls face as a result of archaic and oppressive gender norms. Medicine could be a discipline which makes us see human beings afresh, and opens up our mind to human life in a more realistic way, helping us be better doctors who help people be healthier in a holistic way.We know that beauty is only skin deep, but the misogyny surrounding it and self-hate it creates can cut us right down to our bones, as do harmful ideas about women’s bodies and women’s sexuality, which deeply impact mental health and in turn the overall health of people. If doctors’ goal is to provide healthcare to women, then it’s time they actually focus on women’s health and women’s rights, not damaging women’s minds and bodies for some misguided cultural ideals. Dr Anamika Pradhan is a practising specialist in Mumbai who has studied at one of the medical colleges in the city and feels strongly about the need to produce more humane and thoughtful doctors who can be agents of change in society.
While one may be inclined to dismiss this as an individual case, the shocking reality is that this doctor isn’t the only one of his kind. There’s a growing medical-corporate-pharma complex that feeds into people’s insecurities and upholds patriarchal ideas of what is appropriate for women’s bodies. It starts off with the insidious and all-pervasive suggestion to be ‘fair and lovely’ and then moves on to the need to have flawless skin, no body hair but luxurious hair on your head, smell like a flower, be slim and always be attractive to men. But it doesn’t end with just a focus on external appearance.There is a vaginal ‘tightening’ product called 18 Again that was advertised for a brief while and still continues to be sold. It talks about how it makes the sex feel like the “first time every time”. It also claims to include gold among its ingredients, as well as Punica Granatum, about which it says on its website: “According to a legend, Punica Granatum grew in the Garden of Eden and the fruit has been used as a folk medicine for thousands of years.” Of course there are plenty such ‘snake oil’ variations being sold to gullible people, but this one actually has gynaecologists endorsing it on their website.Setting aside the tall claims of such products, what is so exciting about a woman’s ‘first time’ that one can market that as something worthwhile? Who is a ‘tight’ vagina meant to be pleasurable for? Clearly, for her male partner. How can we have a conversation about women’s sexual pleasure without talking about a range of topics such as foreplay, relationships issues, male erectile dysfunction? Even the medication for male erectile dysfunction gets marketed as something that will help men regain sexual pleasure, not for women whose partners are unable to get it up!If society, with the premium it places on “purity” and virginity, sees women’s sexuality through the lens of male pleasure and is okay with asking women to do unreasonable things to their bodies, doctors are caught in this cultural web too. The reality is that in 5 years of MBBS and 3 years of post-graduate training (whether in ObGyn or any other field), there is no formal training on issues of sexual health. When it comes to women, the entire focus is on reproduction and in managing pathologies like menstrual disorders and other conditions. The biology of pleasure does not figure in understanding women’s bodies, and this is a cultural bias that shapes the medical field.Has anyone looked at the textbooks we learn from? One of the forensic medicine textbooks defines a virgin as “a female upon whose body the sex act has not been performed” – so only women are virgins, and their role in sex is seen as a passive one, of receivers, not participants. Forensic medicine deals with medico-legal cases (such as rape), and thus this kind of mindset is disturbing.Doctors are taught to do the ‘two-finger test’ (based on the scientifically incorrect idea that a tight vagina indicates that someone hasn’t had sex before, while a lax one means a woman is ‘habituated to sex’) for ‘proof’ of rape in a victim. The logic is that if you are a woman who is used to having sex, then you probably weren’t actually raped. Despite changes in guidelines for examining victims of sexual assault and a Supreme Court ban on the test in 2013, many doctors still continue to use the ‘two-finger test’. Only in May 2019 did Maharashtra remove it from medical textbooks and it is probably the only state to have done so.How does one make the transition from being a 19-year-old fresh medical student who is being taught this, day in and day out, and is studying this and needing to write this as an answer in an exam, to becoming a 27-year-old practising doctor who will be able to recognise that this is objectification and derogatory and that ‘virgin’ is not even a medical topic but a socio-cultural concept created by patriarchy to control women’s sexuality? That, it really has no place in a medical syllabus or application?It is a tough journey to make and most never even bother to think that deeply beyond the overwhelming amount of bio-medical information they need to learn, in the absence of any social and cultural contexts or gender and rights sensitisation.It is a sign of the changing times that there is currently, quite rightly, much being written about the judgemental attitudes of doctors (especially gynaecologists) towards women and their sexual lives.The Supreme Court may have declared the right to privacy, but when will the medical profession learn to respect the privacy and the personal spaces and sexual choices of women? When will medical textbooks stop talking of virginity and two-finger tests and include discussion on the social, cultural and religious environment within which health and health seeking is practised?The medical and nursing professions should ideally be at the forefront of enabling such social change, since they bear witness on a daily basis to the violations that women and young girls face as a result of archaic and oppressive gender norms. Medicine could be a discipline which makes us see human beings afresh, and opens up our mind to human life in a more realistic way, helping us be better doctors who help people be healthier in a holistic way.We know that beauty is only skin deep, but the misogyny surrounding it and self-hate it creates can cut us right down to our bones, as do harmful ideas about women’s bodies and women’s sexuality, which deeply impact mental health and in turn the overall health of people. If doctors’ goal is to provide healthcare to women, then it’s time they actually focus on women’s health and women’s rights, not damaging women’s minds and bodies for some misguided cultural ideals. Dr Anamika Pradhan is a practising specialist in Mumbai who has studied at one of the medical colleges in the city and feels strongly about the need to produce more humane and thoughtful doctors who can be agents of change in society.